Adjacent Tissue Transfer CPT Coding Guideline
- Medycoding Expert

- Feb 21
- 4 min read
Updated: Apr 25
Post Last Updated on 21 Feb 2026
Find all updated guideline for adjacent tissue transfer
What is Adjacent tissue transfer?
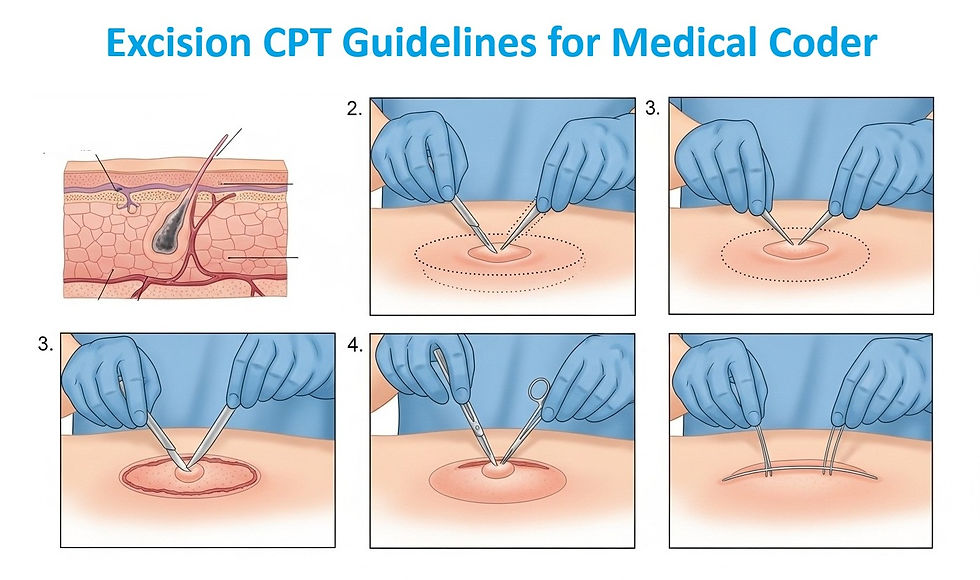
Adjacent tissue transfer refers to a surgical technique in which tissue from an area near a wound or defect is rearranged or moved to cover and repair the affected area.

Calculation of area for Adjacent tissue transfer
What is Primary defect and secondary defect?
The primary defect is the defect that is formed by excision and the secondary defect is the defect that is created during raising the flap for ATT.

What are the Flap technique used by physician in ATT
Z Plasty
W Plasty
V-Y Advancement Flap
Y-V Advancement Flap
Rhomboid Flap
What are the medical necessity of Adjacent tissue transfer?
It is performed to close the defect if surgical repair is not possible to closure the wound.
Adjacent tissue transfer is performed just after the excision to close the defect or later.

What are the alternate term used by the physician in Operative report for ATT ?
Rotated
Advanced
Transpose
Dont confuse with Tissue or Flap is raised, until it is rearranged to surrouding tissue.
What are the CPT code range for tissue Transfer ?
14000-14350 : Adjacent tissue transfer
14000: Adjacent tissue transfer or rearrangement, trunk; defect 10 sq cm or less
14001: Adjacent tissue transfer or rearrangement, trunk; defect 10.1 sq cm to 30.0 sq cm
14020: Adjacent tissue transfer or rearrangement, scalp, arms and/or legs; defect 10 sq cm or less
14021: Adjacent tissue transfer or rearrangement, scalp, arms and/or legs; defect 10.1 sq cm to 30.0 sq cm
14040: Adjacent tissue transfer or rearrangement, forehead, cheeks, chin, mouth, neck, axillae, genitalia, hands and/or feet; defect 10 sq cm or less
14041: Adjacent tissue transfer or rearrangement, forehead, cheeks, chin, mouth, neck, axillae, genitalia, hands and/or feet; defect 10.1 sq cm to 30.0 sq cm
14060: Adjacent tissue transfer or rearrangement, eyelids, nose, ears and/or lips; defect 10 sq cm or less
14061: Adjacent tissue transfer or rearrangement, eyelids, nose, ears and/or lips; defect 10.1 sq cm to 30.0 sq cm
14301 : Adjacent tissue transfer or rearrangement, any area; defect 30.1 sq cm to 60.0 sq cm
14302: Adjacent tissue transfer or rearrangement, any area; each additional 30.0 sq cm, or part thereof (List separately in addition to code for primary procedure)
CPT Code selection Criteria for Adacent Tissue transfer
Codes 14000-14302 are reported based on anatomical location and defect size.The term "defect" includes the primary and secondary defects, which are measured in square centimeters.
Coding guideline for Adjacent Tissue Transfer
In order to choose the appropriate code, add or sum the area of the primary defect (ie, excision) to the area of the secondary defect (ie, raised flap) to determine the total square centimeter area.
Adjacent Tissue transfer include the Excision, so if excision is peformed and to close that defect ATT is chosen then code only ATT. Excision is inclusive in ATT.
When two or more separate wounds within the same anatomical area are repaired with one adjacent tissue rearrangement procedure, the areas of the defects are added to the area of the raised flap to determine one adjacent tissue rearrangement code.
However, if separate defects within the same anatomical area are repaired separately, ie, each defect is repaired with a distinct adjacent tissue rearrangement, then report an appropriate adjacent tissue rearrangement code (14000-14302) for each site. It would be appropriate to append modifier 59.
If debridement is necessary to perform a tissue transfer procedure, then it is included in the procedure, debridment not need to code.
To close the secondary defect, if additionally any graft or flap is used to close the defect then we can seperately. So, skin grafting can be code seperately if it is not documented in the code description of the the ATT.
If ATT and Complex repair performed together at the same site ,what will you report ?
Since, ATT is more extensive procedure that is performed.
So, only ATT will be coded.
Extensively undermining of adjacent tissue to achieve closure of a wound or defect may constitute complex repair, not tissue transfer and rearrangement.
Coding scneario for ATT
Scenario 1: A 4 sq cm basal cell carcinoma is excised from the cheek.
A rotational flap is created by raising 6 sq cm of adjacent tissue to close the defect.
What will be the total size of ATT ?
Answer: Primary defect = 4 sq cmSecondary defect = 6 sq cmTotal area = 10 sq cm
Code selection based on 10 sq cm, not just 4 sq cm.
Scenario 2: Surgeon excises 3 cm malignant lesion on forehead.A bilobed flap is performed to close defect. How will you report
Answer: Do not code excision separately.
Report only ATT code (14040 range depending on size/location).
Scenario 3: Two separate lesions removed from right cheek:
Defect 1 = 2 sq cm
Defect 2 = 3 sq cm
One large rotational flap of 8 sq cm is used to close both.
Answer: Total area:2 + 3 + 8 = 13 sq cm.
Report ONE ATT code based on 13 sq cm.
Scenario 4: Two lesions removed from right cheek:
Defect 1 closed using rotational flap (5 sq cm)
Defect 2 closed using advancement flap (4 sq cm)
Two distinct flaps performed
Answer: Report two ATT codes.
Append modifier 59 to second code
Scenario 5: Nasal lesion excised.
Large rotational flap used to close primary defect.
Secondary donor site defect too large → surgeon applies full-thickness skin graft.
Answer: Code for :
ATT code (primary repair)
Skin graft code (separately)
Because graft is not bundled in ATT description.
Common Surgery Interview question from ATT
1.What is ATT ?
2.How to calculate ATT ?
3.What is primary and secondary defect ?
4.How to report ATT with excision or ATT with complex repair ?
5.Can you code debridement along with Adjacent tissue transfer ?


Comments